Rational approach to sufficient depuration
with minimal set of periodontal instruments
Treatment case by RDH Tatiana Brandt
Introduction
Case for rational approach to sufficient depuration with a minimal set of periodontal instruments
Efficacy of nonsurgical periodontal instrumentation depends on many factors, including gingival inflammation, root anatomy and pain management. However, clinicians’ experience, skills and understanding of periodontal pocket anatomy and defect morphology play a crucial role in the success of subgingival instrumentation. Detailed knowledge of instrument design might also affect technique.
The choice of periodontal instruments for debridement and scaling depends on the location, hardness and composition of tartar, the consistency of adjacent soft tissues, and the topography of the periodontal pocket. Still, it is possible to increase instrument efficiency by selecting appropriate instruments and scaling techniques or better adaptation and movement of instruments.
My choice of hand instrument set will illustrate a professional approach to a time-effective and rational use of only a few periodontal instruments. The suggestion of instrument set aims to meet individual clinicians’ needs and references, and in addition to this, is designed to adjust the choice of instruments to reflect the extent and severity of patients’ diseases.
Working with step-by-step illustration of specific set of instruments will help clinicians to systematize the approach to periodontal instrumentation, give suggestions on how to be more creative in instrument choice and application, make instrument use more beneficial for root sites with concavities, grooves and depressions, and be less time-consuming. Besides, novice clinicians often find it helpful to review a simple instrumentation guide.
It is advisable to perform sub-gingival periodontal hand instrumentation in combination with powered ultrasonic instrumentation, considering that instrument condition and sharpness are critical in providing successful periodontal treatment. My desire is to show, through step-by-step clinical cases, how various instruments are used in practice to produce outstanding treatment results. This periodontal set illustrates treatment case with short explanatory texts alongside the images. I have selected the periodontal set based on size and location of tartar deposits, root topography, and an individual clinician’s preferences together with an idea of a rational approach, without compromising quality.
The choice is still the clinician’s choice. There are many excellent options and other plans for tartar removal that can be developed by experienced dental professionals.
Treatment case
Rational approach to sufficient depuration with minimal set of periodontal instruments: Effective instrumentation with LM™ Dual Gracey curettes
Text and clinical pictures by RDH Tatiana Brandt, clinical lecturer at School of Oral Health Care, University of Copenhagen
Effective periodontal instrumentation may be achieved by using just a few instruments, provided that the correct
instrumentation technique is used. There are many combinations of technical depuration solutions with a minimal number of hand instruments, but the clinician’s preferences are the most important factors in choosing the optimal set of instruments.
This set is for dental professionals who prefer working with universal curettes but also need a subgingival approach. LM Dual Gracey™ instruments, also known as Syntette™, combine traditional universal curettes and Gracey curettes to provide efficient supragingival instrumentation and allow subgingival access in deep pockets.
Video
Above you find the treatment case presented on this page as full step-by-step demonstrational video.
PDF document
You can also download the full illustrated case as PDF document.
Clinical characteristics
When planning tartar removal, some questions need to be answered: What anatomical characteristics present a challenge for this patient? What type and size of tartar has been detected? What type of gingival phenotype does the patient have: thin or thick? Which of the periodontal instruments should you select for removing tartar from the front and back teeth?
The present case demonstrates an instrumental approach to patients with the following clinical characteristics:
- Treatment of patient with small to moderate tartar deposits
- Probing depth ≤ 5 mm
- Patient with gingivitis or periodontitis
- Vertical and horizontal bone loss may occur
- Some gingival recession may occur
- There may be furcation involvement
This case does not take account of periodontal diagnostics.
The gingiva has been removed from the typodont in this case images, to provide a view of the working-end of the instruments.
Choice of instruments
My choice for this severity level is a set of LM Dual Gracey™ curettes, a sickle and a universal curette.
- Mini Syntette™ Anterior SD: a combination of universal curette and Mini Gracey 1/2 and Mini Gracey 7/8 curettes
- Mini Syntette™ (posterior) SD: a combination of universal curette and Mini Gracey 11/12 and Gracey 13/14 curettes
- Sickle LM23 SD (alternative Mini Sickle SD)
- Barnhart 5-6 SD

Figure 1 Instruments with sharpen-free LM Sharp Diamond™ coating: Mini Syntette™ Anterior SD 275-276MSDES, Mini Syntette™ SD 215-216MSDES, Sickle LM23 SD 313-314SDES and Barnhart 5-6 SD 227-228SDES.
Related products


All chosen instruments are sharpen-free LM sharp Diamond™ (SD) coated instruments. Delicate working blades are quite difficult to sharpen and the lifetime of mini-model LM Sharp Diamond™ instruments is longer compared to stainless steel instruments.
Gracey curettes are available in standard, mini, macro and rigid model versions. Rarely are all Gracey curettes used by the clinician at the same appointment. A set of three or four suitable instruments may be enough to instrument an entire dentition. Even working rationally, as an experienced clinician, you will commonly need at least two to three double-ended Gracey curettes for periodontal instrumentation of back teeth. When the gingiva is inflamed, soft, thin and bleeding, something you can see at the first initial treatment stage of the patient’s periodontitis will be needed.
The higher cutting edge of the Gracey curette, angled away from the soft tissue wall, is an advantage,
especially while working with very inflamed thin biotypes of gingiva. Scaling the well treated maintenance patient or a patient with gingival retraction is easier to manage due to reduction in bleeding, the small amount of newly emerged tartar and firmer soft tissue.
On the basis of the above, working with Syntette™, that is, LM Dual Gracey™ instruments instead of Gracey curettes will be a more rational choice and the clinician’s work will become more time-efficient. These instruments can be adapted to mesial and distal tooth surfaces alike without changing instruments. Each LM Dual Gracey™ tip has two elliptical cutting edges, a mesial and a distal edge. The lower shank must be kept parallel to the tooth surface during scaling. LM Dual Graceys™ are suitable for vertical, horizontal and oblique scaling techniques. The face of a working blade is not suitable for scaling the bottom or ceiling of furcation areas and needs an additional instrument.
.
It is necessary to understand the differences and similarities between Syntette™ and Gracey curettes in order to choose the appropriate Syntette™ version and the right additional universal instrument either for removing plaque from furcation areas and finishing strokes or for removing tartar. Mini Syntettes™ are suitable for light scaling and plaque removal in periodontal maintenance patients with tight pockets. Standard Syntette™ is better recommended in the same combination with Barnhart 5-6 and Sickle LM23 for initial periodontal treatment and for removing more substantial tartar deposits.
Mini Syntette™ Anterior is designed for removal of supra[1]and sub-gingival tartar in premolar and anterior areas, for all tooth surfaces. It is especially suitable for scaling grooves, concavities and depressions on mesial and palatal sites. Additionally, it can be used on straight root surfaces in furcation areas, but not on furcation area ceilings or bottoms.
Mini Syntette™ (posterior) is designed for removal of supra and sub-gingival calculus in premolar and molar areas, for all tooth surfaces. Additionally, it can be used on root surfaces in furcation areas, but not on furcation area ceilings or bottoms. Mini models are excellent in narrow and deep pockets in maintenance patients.
Barnhart 5-6 is designed for molars and is used in this case for light scaling of furcation area ceilings and bottoms. It can also be used as a universal curette in a whole tooth set, if deposits are predominantly small and located just under the first 3 mm of gingiva.
Sickle LM23 (alternative Mini Sickle) is for finishing and evaluating vertical strokes in front and back proximal spaces and for fracturing of any burnished tartar.
Effective instrumentation with LM Dual Gracey™ curettes
It is always preferable to start removing medium-size calculus deposits above and below the gingival margin with a powerful ultrasonic instrumentation, choosing a tip designed to be more active at moderate power settings followed by hand instruments. If tartar is tenacious, it would be appropriate to use some vertical movements with a first third-part of the scaler tip to fracture the tartar before using Gracey curettes. However, this case describes a recall patient with small tartar deposits. It is advisable to apply periodontal instrumentation from the distofacial line angle to the midline of the distal surface on molars and premolars. I prefer starting from the first quadrant and continuing to make a series of short, precise strokes across the distal surface using Mini Syntette™ (posterior). Watch the bend between the lower and upper shank; it is pointed distal as shown in Figure 2a. Use a series of precise overlapping horizontal and oblique strokes for the distal and facial surface of the back teeth, beginning at the distofacial line angle (Figure 2b).
Horizontal strokes are very effective in removing deposits from the distal line angle of back teeth. The third tip adaptation of the working end is the same as with Gracey, parallel to the tooth. The adjustment of lateral pressure depends on your fulcrum and your stroke technique.

Figure 2a Scaling with Mini Syntette™ (posterior) SD of molar and premolar distal surfaces (vertical strokes).

Figure 2b Scaling with Mini Syntette™ (posterior) SD of molar and premolar distal surfaces (horizontal strokes).
Move on and continue instrumentation at least halfway across the mesial surface from the facial aspect using the same working end of Mini Syntette™ (posterior). Then use some horizontal facial strokes if necessary and if the soft tissue is quite loose. Horizontal strokes are also effective when a neighboring tooth is missing, as depicted (Figure 3b).

Figure 3a Scaling with Mini Syntette™ (posterior) SD of molar and premolar mesial surfaces (vertical strokes)

Figure 3b Scaling with Mini Syntette™(posterior) SD of molar and premolar distal surfaces (horizontal strokes)

Figure 3c Scaling with Mini Syntette™ (posterior) SD of molar and premolar mesial surfaces (horizontal strokes)
Proceed to the palatal or lingual side with the same instrument, using another working end if necessary. Place the Mini Syntette™ (posterior) with the toe pointing toward the mesial surface and gently slide the working end under the gingival margin. Make a series of horizontal overlapping strokes in the mesial direction.

Figure 4a, Scaling with Mini Syntette™ (posterior) SD of molar and premolar palatal and lingual surfaces (horizontal strokes)

Figure 4b Scaling with Mini Syntette™ (posterior) SD of molar and premolar palatal and lingual surfaces (horizontal strokes)
Furcation areas can be scaled with a combination of two instruments: Mini Syntette™ (posterior) and Barnhart 5-6 (Figures 5a, 5b, 5c and Figures 6a, 6b, 6c).
Note the different fulcrum position and application of different lateral pressure using Mini Syntette™ and Barnhart 5-6. It is advisable to use very light strokes in the bottom and ceiling of furcation areas, occasionally using a diamond file for extra polishing.
Completing a maxillary and mandibular quadrant on one side of the mouth before proceeding to anterior teeth is recommended, especially when local anesthesia is indicated for two quadrants, because the maxillary arch can be more difficult to scale.

Figure 5a Scaling with Mini Syntette™ (posterior) SD of distal and mesial root aspects of furcation area (vertical strokes)

Figure 5b Scaling with Mini Syntette™ (posterior) SD of mesial root aspects of furcation area (vertical strokes)
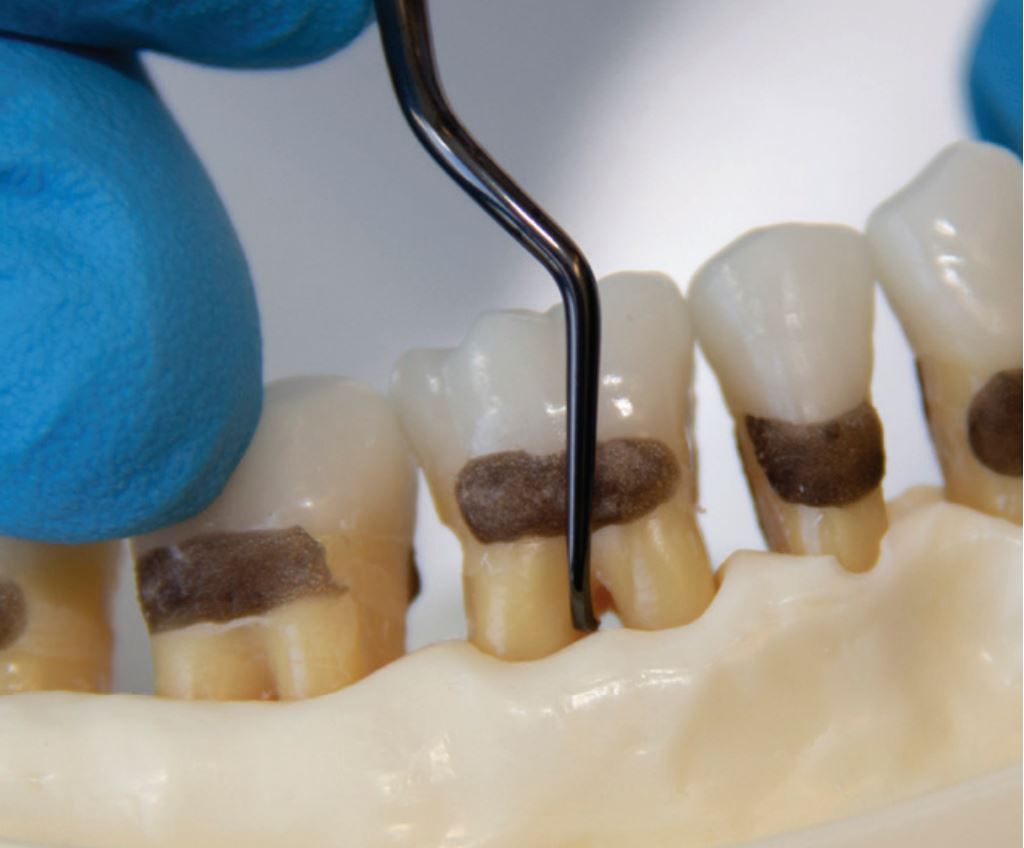
Figure 5c Scaling with Mini Syntette™ (posterior) SD of mesial root aspects of furcation area in lower jaw (vertical strokes)

Figure 6a Scaling of ceiling of furcation area with Barnhart 5-6 SD using very light strokes

Figure 6b Scaling of ceiling of furcation area with Barnhart 5-6 SD using very light strokes

Figures 6c Scaling of ceiling of furcation area with Barnhart 5-6 SD using very light strokes
Instrumentation of the front teeth is possible, starting with scaling all surfaces facing you, then flipping the instrument and scaling all surfaces facing away from you on the facial. Figures 7a and 7b depict application of the cutting edges to the maxillary front teeth, facial aspect.

Figure 7a Scaling of front teeth with Mini Syntette™ Anterior SD (vertical strokes towards clinician, facial and palatal aspect

Figure 7b Scaling of front teeth with Mini Syntette™ Anterior SD (vertical strokes away from clinician, facial and palatal aspect

Figure 8a Scaling of retroclinated front teeth with Mini Syntette™ (posterior) SD
It can be appropriate to use Mini Syntette™ (posterior) on front teeth that are inclined backwards (retroclinated) when the angulation of Mini Syntette™ Anterior is difficult.
A common scaling mistake occurs when scaling strokes with mini model instruments do not extend past the midline of the proximal surfaces. It is therefore advisable to finish instrumentation by doing some vertical evaluating strokes on proximal root surfaces and some scaling strokes under the contact points, using a sickle scaler. A sickle is very good for removing tenacious tartar because of its strong, rigid working end and pointed tip, which provides a good access to proximal surfaces.
Although the sickle is not recommended for use on root surfaces, it is excellent for detective evaluating strokes and removal of small pearls of tartar on the middle part of distals and mesials. In this case, the recommended device is Sickle LM23 (Figures 9a, 9b, 9c) with shorter blades and longer lower shank than in the Mini Sickle for periodontal patient maintenance.

Figure 9a Scaling of back teeth with Sickle LM23 SD vertical detecting strokes)

Figure 9b Scaling of front teeth with Sickle LM23 SD (finishing vertical strokes)

Figure 9c Scaling of front and back teeth with Sickle LM23 SD (finishing detecting horizontal strokes)
As an alternative, the Mini Sickle can be used for the same purpose. When doing short powerful vertical strokes in proximal, the fulcrum in the lower jaw is further behind the working area. Use very short precise fracturing horizontal strokes if the tartar is too tenacious. Only 1-2 mm of a tip is used, to avoid soft tissue trauma (Figures 10a, 10b).

Figure 10a Detective evaluating strokes with Mini Sickle SD as alternative to Sickle LM23 SD (vertical strokes

Figure 10b Detective evaluating strokes with Mini Sickle SD as alternative to Sickle LM23 SD (horizontal strokes)
To provide a better spooling effect, and to remove the tiniest deposits at the bottom of the pocket, a slim periodontal ultrasonic tip, preferably 40H, can be additionally used following evaluation with an Explorer 11-12.
Clinician
Tatiana Brandt
Text and clinical pictures by RDH Tatiana Brandt, clinical lecturer at School of Oral Health Care, University of Copenhagen
About me:
- Tatiana Brandt, RDH Med (Master Degree in Health Education and Health Promotion)
- I have been practicing clinical dental hygiene for 17 years, and worked for the Department of Odontology and Periodontology at the Copenhagen School of Dentistry.
- Board member of Danish Society of Periodontology.
- For the last 10 years, I have been clinical lecturer at the School of Oral Health Care, Faculty of Health and Medical Science, University of Copenhagen.
- Speaker and course provider for LM-Dental™ and Plandent.
- My main interest is advanced periodontal instrumentation, ergonomics and prevention of MSD in hands and wrists.